
Advanced medical technologies rarely fail because of what they can do — they fail because of how they are adopted. Over the past two decades, we have seen the same pattern repeat itself across hospitals of all sizes and geographies. A new technology is acquired with enthusiasm, often backed by strong clinical promise and significant capital investment, only for it to underperform within months. Utilization drops, outcomes become inconsistent, and what was initially positioned as a strategic leap forward gradually turns into an underused asset.
The issue is rarely the technology itself. More often, the failure lies in how it is introduced, integrated, and supported within the clinical environment.
The Procurement Trap
Many institutions approach advanced technologies as procurement decisions rather than programmatic ones. The focus is placed on specifications, pricing, and vendor comparisons, while the more important question: how this technology will be used in practice, is left insufficiently defined.
In reality, technology should follow clinical intent. Programs that succeed begin with a clear understanding of where the device will add value, which patient populations will benefit, and which physicians are prepared to adopt it. Without this foundation, even the most advanced systems struggle to find a meaningful role in daily practice. (For a concrete example of this principle in action, see how to launch a surgical robotics program.)
The Illusion of Training
Another common misconception is that training is a discrete event rather than a continuous process. A workshop is conducted, a few initial cases are performed, and the assumption is that the team is now “ready.”
In practice, this is where the real work begins.
Skill acquisition in complex procedures is incremental. It requires repetition, feedback, and structured progression. More importantly, it requires alignment across the entire team: surgeons, anesthesiologists, nursing staff, and technical support. When training is treated as a checkbox rather than a pathway, variability increases, confidence declines, and the technology is often abandoned before proficiency is reached.
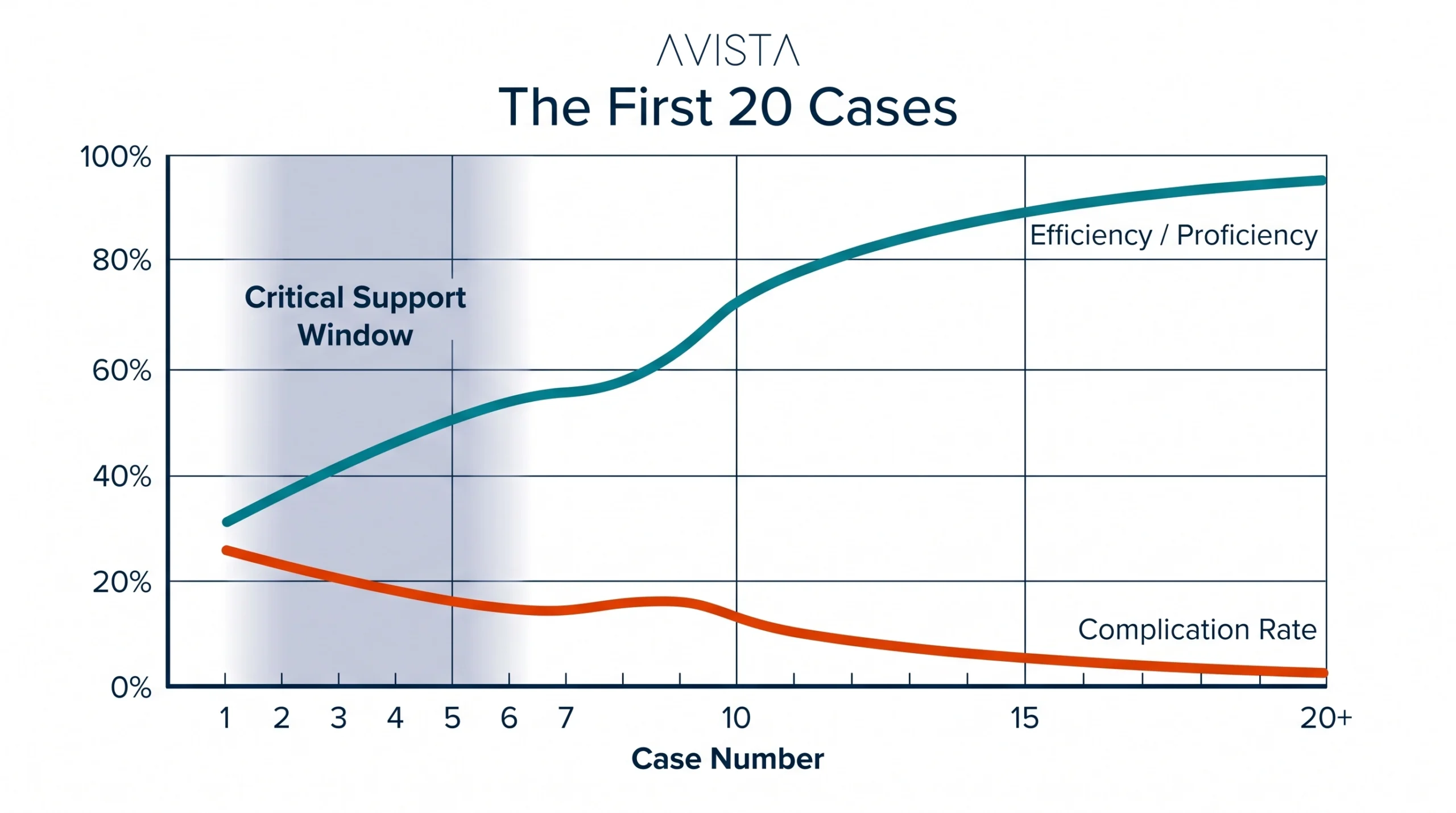
The First 20 Cases
If there is a single phase that determines the fate of a new program, it is the early case experience. The first 20 procedures are where teams encounter unfamiliar anatomy, unexpected technical challenges, and the limits of their preparation.
Without appropriate support during this phase, whether through proctorship, experienced clinical specialists, or structured oversight, the likelihood of complications rises. Even when outcomes are acceptable, inefficiencies can erode confidence among both clinicians and administrators.
The programs that endure are those that treat these early cases with discipline. Patient selection is conservative, support is readily available, and there is a clear willingness to adjust strategy when needed. This phase is not about demonstrating capability; it is about building it.
Utilization: The Silent Determinant
One of the most overlooked aspects of program success is utilization. Advanced technologies require consistent use to justify their presence, not only financially, but clinically. Skills degrade without repetition, workflows remain inefficient, and teams never reach a level of comfort that allows the technology to deliver its full benefit.
Low utilization is rarely a result of insufficient demand. More often, it reflects a lack of structure: unclear case selection, limited surgeon engagement, or operational barriers within the hospital.
Sustainable programs are built around predictable case volumes. They begin with procedures that are reproducible and gradually expand into more complex indications. Over time, this creates a rhythm within the system, where both clinical and operational teams function with increasing efficiency.

The Invisible Layer: Technical and Engineering Support
There is a layer of program success that is often underestimated, largely because it operates in the background. Technical readiness, device handling, troubleshooting, and system maintenance all play a critical role in ensuring consistency.
When this layer is weak, problems tend to surface at the worst possible time: during procedures. Delays occur, confidence is disrupted, and the perception of the technology shifts from enabling to burdensome.
Strong programs invest in this infrastructure from the beginning. Biomedical teams are trained, protocols are established, and there is clarity around how issues will be managed when they arise. This is not simply an operational consideration; it is a clinical one. (We explore this layer in depth in why most MedTech value is
delivered after installation.)
Data as a Driver of Maturity
Programs that succeed over the long term are those that develop the discipline to measure themselves. Operative times, complication rates, conversion rates, and cost per case are not just administrative metrics: they are indicators of how well the system is functioning.
When tracked consistently, these data points provide insight into where improvements can be made. They allow teams to refine workflows, identify learning gaps, and make informed decisions about expansion.
More importantly, they create accountability. In the absence of data, perception often replaces reality. With data, progress becomes tangible.
Building Programs, Not Installing Devices
The distinction between failure and success in advanced medical technology is rarely dramatic. It is incremental. It lies in the accumulation of small decisions: how patients are selected, how teams are trained, how early cases are managed, and how consistently the system is used.
Hospitals that approach these technologies as isolated purchases tend to struggle. Those that view them as long-term programs, requiring structure, discipline, and ongoing investment, tend to succeed.
The difference is not in what they buy, but in how they build.
Closing Perspective
Advanced medical technologies have the potential to redefine clinical practice. They can expand what is possible, improve patient outcomes, and elevate the standard of care. But they do not do this on their own.
Their success depends on the environment into which they are introduced.
In the end, the question is not whether a technology works. It is whether the system around it is designed to make it work: consistently, safely, and at scale.
Frequently Asked Questions
Why do advanced medical technologies fail after launch?
Rarely because of the technology itself. The most common causes are treating acquisition as a procurement decision rather than a program, one-off training, weak early-case support, and low utilization.
Why are the first 20 cases so important?
They are where teams meet unfamiliar anatomy, technical surprises, and the limits of their preparation. Structured support in this window largely determines whether the program builds momentum or stalls.
What does sustainable utilization look like?
Predictable case volumes, starting with reproducible procedures and expanding gradually — so skills, workflows, and confidence grow in parallel.
Avista builds the support layer this article describes — clinical specialists for early cases, structured training pathways, and technical readiness programs. Talk to our team before your next technology launch.










